Spondylolysis-Isthmic Spondylolisthesis
History Summary
- 23 year old man
- Professional Footballer
- Had to quit playing because of Severe Right-Sided Lower Back Pain
- Extensive Physiotherapy - No help
- Pain management failed
![]()
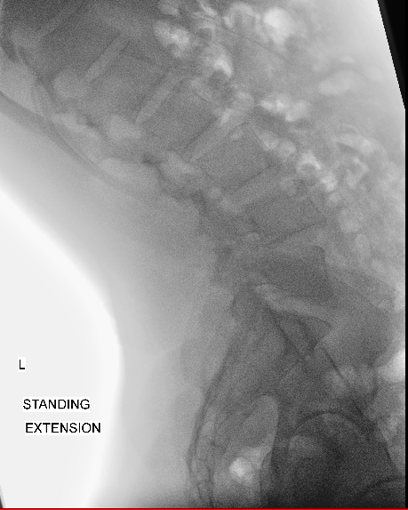
The patient was a 23 year old professional footballer who was forced to quit playing because of severe right sided lower back pain. Extensive physiotherapy and Pars injections had failed to improve his pain.
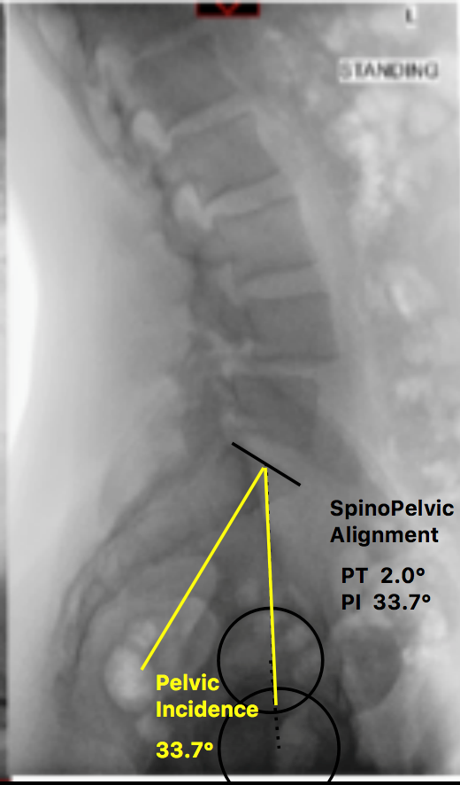
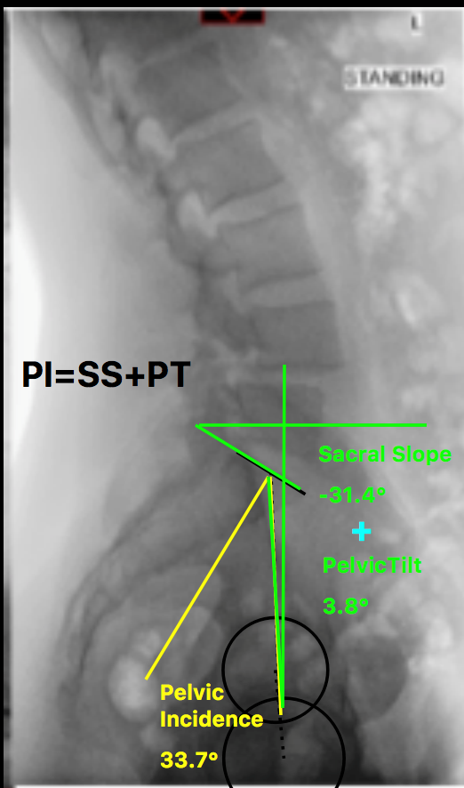
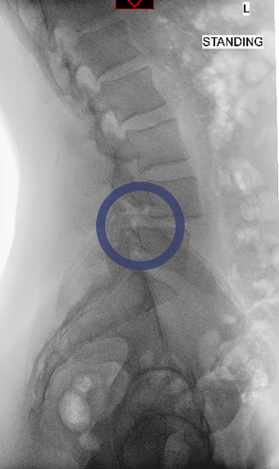
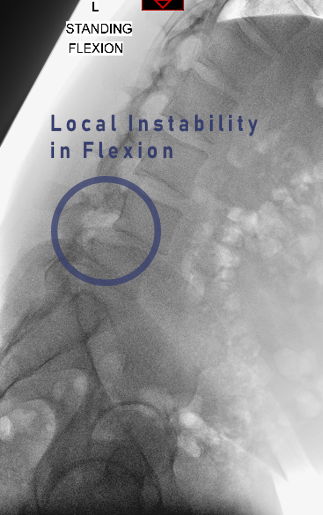
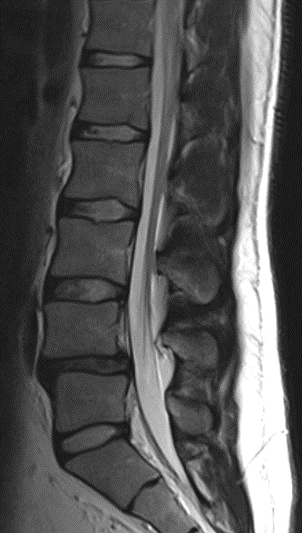
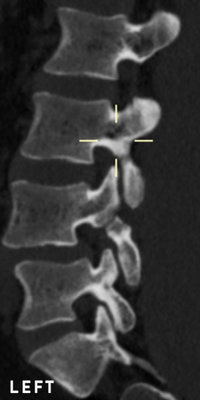
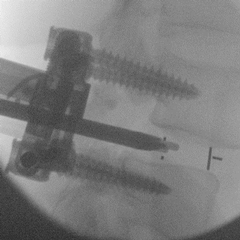
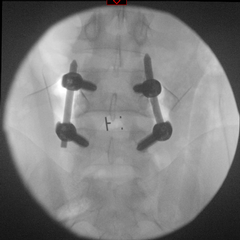
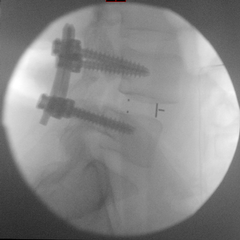
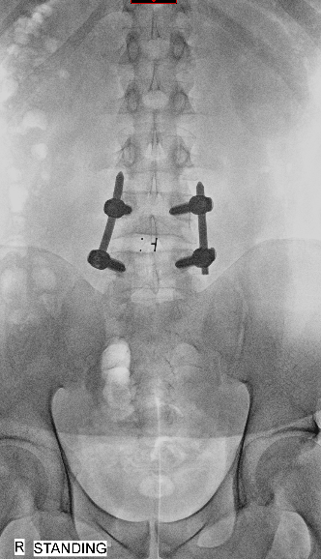
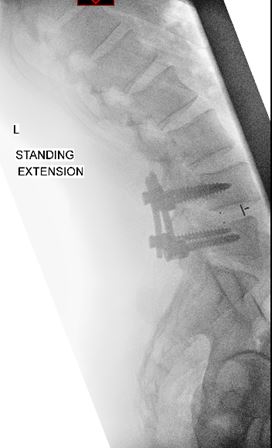
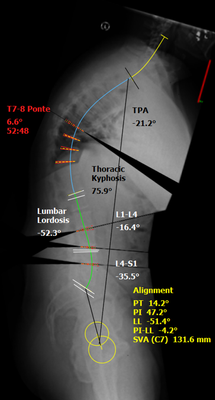
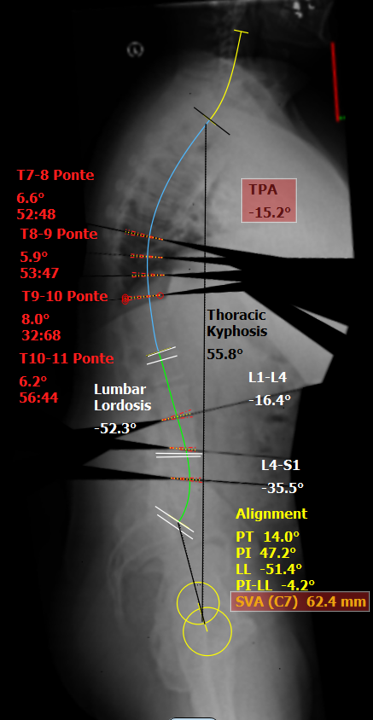
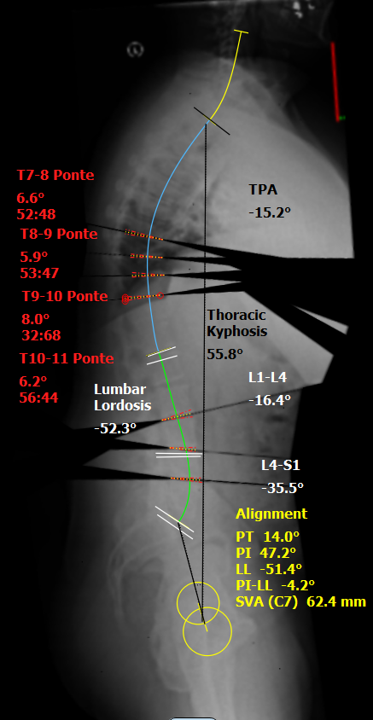
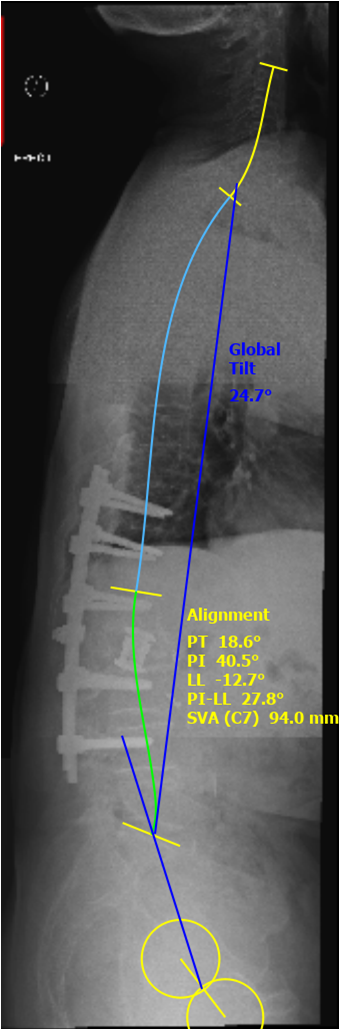
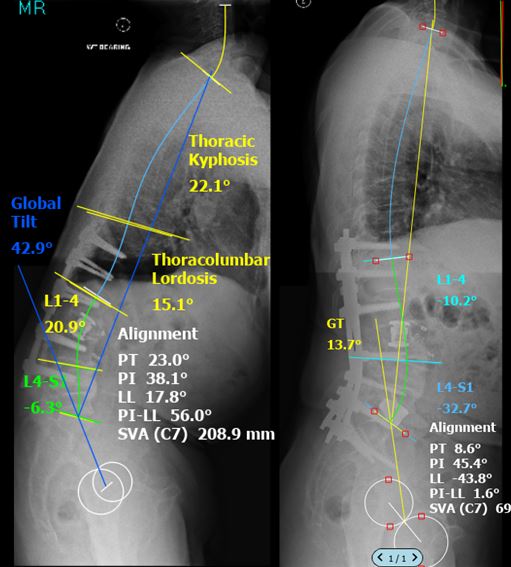
Lumbar spine X-rays revealed that the patient was suffering from Grade I Isthmic Type Spondylolisthesis. After failure of nonoperative treatments the patient underwent an MIS Transforaminal Interbody Fusion (MIS TLIF). Immediately after surgery his pain has resolved.
Six months after the operation following extensive post-operative rehabilitation he returned to playing football.